Introduction
Reminder of observations:
| Age | RR | HR |
| 0-2 | 30-40 | 80-180 |
| 2-12 | 20-30 | 60-140 |
| 12+ | 12-20 | 60-100 |
Quick formula for blood pressure:
50th Centile for blood pressure in children > 1 year =
90 + 2(Age in Years) mm Hg
Important considerations in Paediatric Trauma:
- Accidents and injuries are the second most common cause of mortality and morbidity in children and adolescents (1).
- Children are more likely to have hidden internal trauma than adults due to:
- Reduced muscle mass
- Reduced subcutaneous fat
- Increased elasticity of bones
- Intracranial Trauma is responsible for 70% of deaths in first 48 hours post trauma
- A triad of Acidosis, Hypothermia, and Coagulopathy significantly increases mortality
The following article will cover the initial A-E assessment in paediatric trauma, with the approach of:
- Primary Survey + Resuscitation
- Imaging Series – Chest & Pelvis
- A C-spine X-ray may be part of secondary survey depending on the circumstances. Some centres may perform a Trauma CT (Head, Neck, Chest, Abdo, and Pelvis)
- Secondary Survey
- Emergency treatment
- Definitive Care
Primary Survey
Use a modified version of ABCDE -> <C>AcBCDE approach
| Treat first what kills first | |
| <C> | Catastrophic External Haemorrhage |
| Ac | Airway + C-Spine |
| B | Breathing |
| C | Circulation |
| D | Disability (AVPU, Pupils, Posture) |
| E | Exposure |
A systematic approach to assessing a child with trauma will allow you to identify the most significant/ life threatening injuries in an efficient manner.
- Put out a paediatric trauma call as soon as possible – the trauma team usually (but not always) includes a member of the ED, paediatric, surgical, orthopaedic, and anaesthetic teams.
- It is important to attach monitoring as soon as the child arrives.
<C>: Catastrophic Haemorrhage
This refers to external bleeding that will lead to death without immediate management. It is often caused by penetrating trauma e.g. knife injury, blast injury, gunshot injury. In many parts of the world, this is less common than blunt force trauma.
Management
- Apply direct pressure
- Ideally with haemostatic dressing
- Consider torniquet above wound if on limb
- Activate your hospital’s major haemorrhage protocol – this will alert the labs to start preparing and dispensing blood products
- Blood products
- Red Cells + FFP in 1:1 ratio
- Consider use of cryoprecipitate and platelets
- Give Tranexamic Acid (Anti-fibrinolytic)
- Red Cells + FFP in 1:1 ratio
Ac: Airway + C-spine
Airway
If concerned about a C-Spine injury, ensure the C-Spine is immobilised/protected prior to performing any airway opening manoeuvres. This can be achieved with ‘manual in line stabilisation’ or by using a headblock and strapping.

Is the airway patent?
- Are they talking?
- Can you hear any upper airways sounds? E.g. stridor or snoring
- Can you see any debris in the airway?
- Remove under direct vision if visible
- See-Saw breathing
If airway is not patent OR you’re worried about it:
Manoeuvres
Try jaw thrust
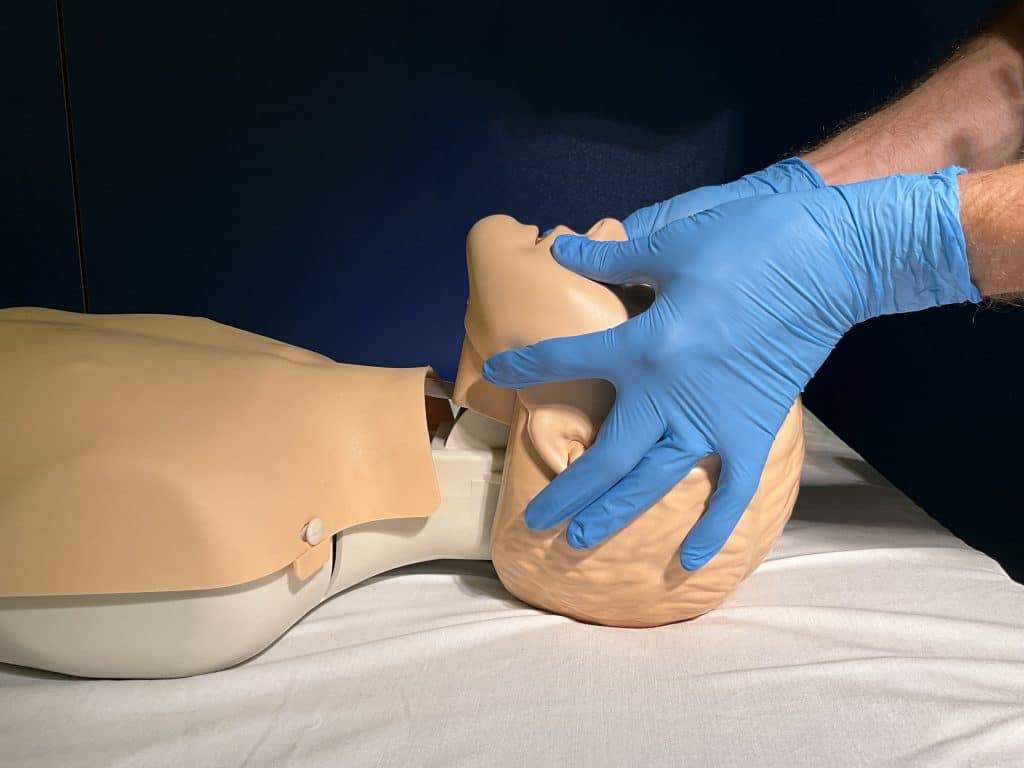
AIRWAY is priority here so it may be necessary to slightly extend neck to open airway
- Remember for infants the position is neutral, children is sniffing air
Adjuncts
Oropharyngeal Airway (OPA)
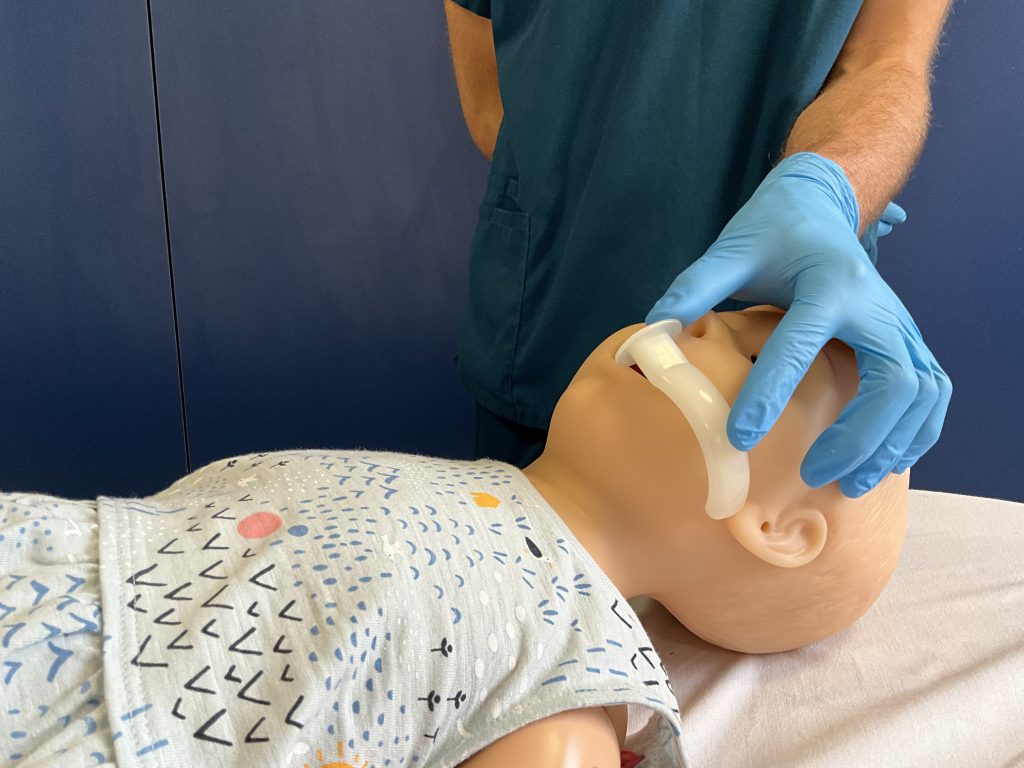
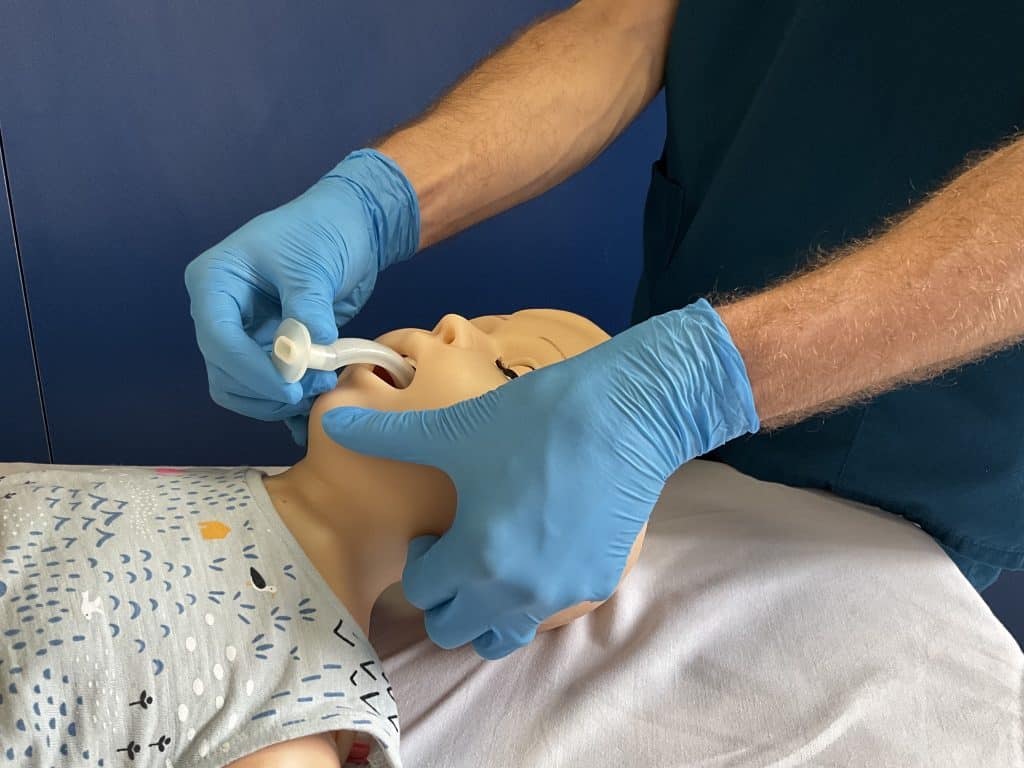
- If the child does not gag or respond to it, this indicates a lack of gag reflex and intubation should be considered
- This does not protect from aspiration
Supraglottic airway
- Consider if even with OPA airway still isn’t open, or ventilation is difficult
- Provides better ventilation than OPA and can attach oxygen directly to it
- Still not a definitive airway and doesn’t protect from aspiration
Nasopharyngeal airway
- Avoid in trauma as there may be a basal skull fracture you haven’t spotted yet
Intubation
This is considered when:
- Manoeuvres and adjuncts are not enough
- You think they’re going to need ventilation for a while
- Inhalation injury
- Decerebrate/decorticate posturing
- GCS<8
C-spine
Children are more prone to C-spine injuries as they have easily compressed soft tissues, more flexible joints, and more elastic ligaments.
C-spine injuries can present normal on imaging known as Spinal Injury Without Radiological Abnormality (SCIWORA). If you clinically suspect it, treat as C-spine injury.
During the primary survey, minor lateral elevation (up to 45 degrees) can be done to look for injury, but no formal log roll should be completed until the pelvis is cleared.
Headblocks can be used to stabilise the C-spine, therefore freeing up a team member.
- During intubation, blocks can get in the way so they need to be removed and manual inline stabilisation should be completed.
- Young children may not tolerate headblocks, so may need manual inline stabilisation – involve the parents in calming the child down.
- Evidence for the use of spinal collars is controversial. It is no longer recommended by UK Resus council, but use your local guidelines.
B: Breathing
| Age | RR |
| 0-2 | 30-40 |
| 2-12 | 20-30 |
| 12+ | 12-20 |
- Aim for O2 sats 94-98% during resus
- Are they breathing? (Check for up to 10 seconds)
- Look – Chest rising, O2 mask fogging up or valves moving?
- Listen – Can you hear breathing or any abnormal noises e.g. grunting or snoring
- Feel – Either place your ear next to the mouth, or use your wrist near the mouth
Concerning breathing signs:
- Nasal flaring in infants/tracheal tug in toddlers
- Is the Trachea deviated?
- Grunting
- Subcostal or Intercostal recessions
- Accessory muscle use e.g. Abdomen or trapezius
- Respiratory rate being too high, too low, or an abnormal pattern e.g. See-Saw breathing

Tension Pneumothroax
This happens when a one-way valve is formed in chest wall so air can enter but not leave, for instance due to stab wounds.
Signs
- Hypoxia
- Absent/decreased sounds on affected side
- Tracheal deviation away from affected side
- Cardiac complications of high-pressure compression on mediastinum
- Distended neck veins
- Tachycardia
- Drop in blood pressure
Management
Needle Thoracocentesis (Inserting a cannula into the chest)
- 2nd intercostal space mid-clavicular line (MCL) – Easiest
- 5th intercostal space mid-axillary line (MAL)

- If still using a bag valve mask (BVM), keep the cannula uncapped, whereas if the patient is breathing, cap the cannula until the chest drain is in place.
If you are worried about breathing, take a blood gas. This will be useful for now and later stages of the primary survey.
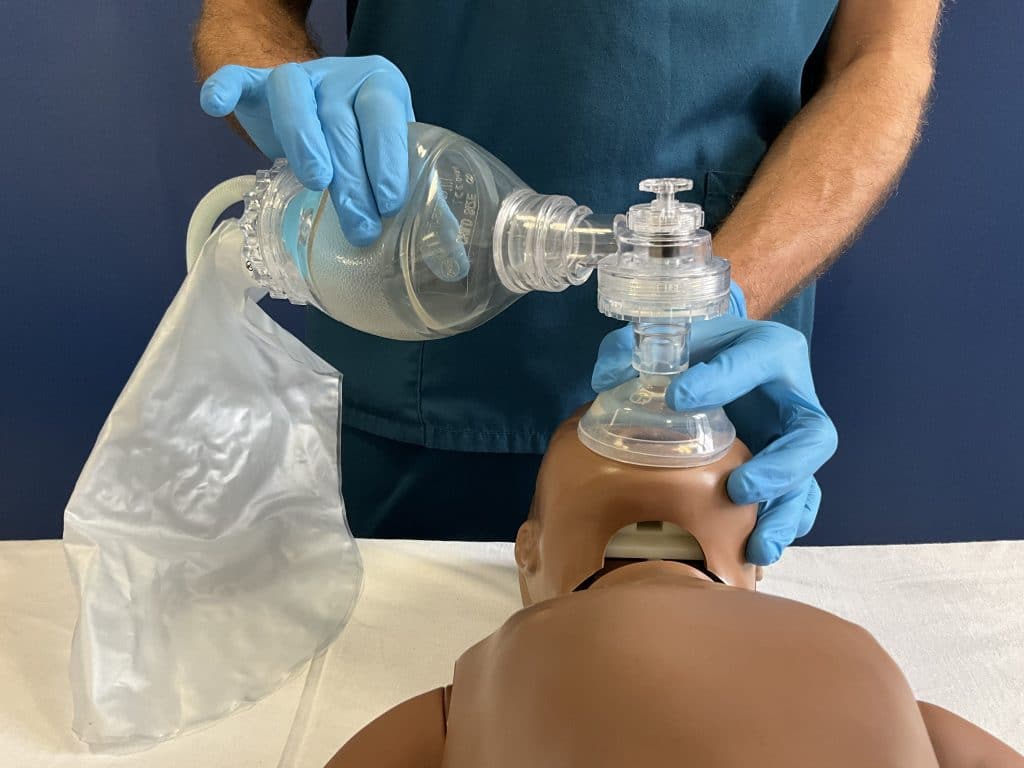
It is important to look out for gastric distention which can occur due to BVM ventilation. If you are worried about it, or the child is intubated, then insert a gastric tube by the oral route.
C: Circulation
| Age | HR |
| 0-2 | 80-180 |
| 2-12 | 60-140 |
| 12+ | 60-100 |
Signs of poor dehydration status
By looking:
- Pale/Blue/Mottled
- Dry mucous membrane
- Lack of tears
- Drowsy/confused
By feeling:
- Cold
- Weak radial and carotid pulse
- In infants use the brachial and femoral pulses
- Obs
- Tachycardia
- Low blood pressure (this is a late stage sign)
Where to look for blood:
Use the phrase: On the floor, four more, and behind the door
- On the floor
- Any external haemorrhage?
- Four more
- Chest, Abdo, Pelvis, or long bones: Have a feel of these areas to feel for fluid or swelling.
- Behind the door
- Retroperitoneal
- Depending on your facilities, may be able to do a POCUS Ultrasound
- Negative USS does not rule out bleeding – the definitive imaging is CT angiography.
Important note: Closed head trauma is not associated with hypovolaemia as not a large amount of blood can collect there. If a patient is shocked, they are bleeding from somewhere else too.
How to manage:
- Two large bore cannulas and take bloods
- Blood gas if not taken already
- Group and save, Cross-Match, FBC, Glucose, LFT, U+Es
- Consider troponin in chest trauma or creatinine if worried about a crush injury
- Fluid resuscitation: 10ml/kg of warm crystalloid
- If inadequate or no response then repeat
- If inadequate or no response to this, follow management from above in <C> section
- If there are concerns about major haemorrhage, it is preferred to use blood products for resuscitation (if available)
- If inadequate or no response then repeat
- Discuss with relevant surgeons/interventional radiology team to decide whether immediate or delayed surgery is indicated. This is relevant if you are working in a major trauma centre or have a surgical team confident with trauma surgery. If not, you may need to consider transfer to a major trauma centre.
D: Disability
This includes assessing:
Level of consciousness:
- Glasgow coma score (GCS)
- AVPU can be used for the immediate assessment:
- A – Alert
- V – Voice (if they wake and react to voice)
- P – Pain
- It is preferred, central pain can be assessed using a trapezius squeeze, supraorbital pressure, or a sternal rub.
- Peripheral pain can also be tested by squeezing the nail bed or earlobes.
- P on AVPU is equivalent to GCS 8 and is an indication for intubation.
- U – Unresponsive to any stimuli
Pupils:
- Pupils should constrict (2-4mm) in response to light, both directly and consensually.
- Unilateral dilation could indicate raised intracranial pressure (ICP) or a brain bleed. It indicates an urgent CT and neurosurgical opinion
Posture:
- Is there decerebrate or decorticate posturing?
DEFG – DON’T EVER FORGET GLUCOSE
If you’re worried at all about neurological status, start 15 minute neuro observations and stretch out as appropriate.
E: Exposure
- Appropriately undress the child to examine whole body looking for any injuries. All children should be covered in between examinations.
- Temperature is very important to check as they may have been lying out in the cold for a long time. This is especially important for infants and babies who rapidly lose heat.
- Remember the triad of increasing mortality: acidosis, coagulopathy, hypothermia
Abdominal injuries
- Expose the abdomen
- Look for any tenderness/ bruising- even a small bruise could be indicative of a significant underlying injury
- Get a urine sample if possible – a urine dipstick that is positive for blood could indicate renal injury
Imaging
Imaging in trauma is a large topic and beyond the scope of this overview article. Some key principles include:
- To keep ionising radiation dose ‘As Low As Reasonably Achievable’ (ALARA) and so routine use of whole body CT is NOT indicated
- Only request CTs that will change management
- In multi-system trauma, a whole body CT (head to pubic symphysis) may be appropriate for critically injured patients
- Primary survey imaging would include a CXR and C-spine x-ray IF it can’t be cleared clinically and there is no indication for C-spine CT
- The need for pelvic x-ray should be considered on a case-by-case basis as children rarely have significant pelvic ring fractures
- Focused Abdominal Sonography in Trauma (FAST) should not be performed if it would delay transfer to CT as CT with contrast is the modality of choice
References
(1) https://stateofchildhealth.rcpch.ac.uk/evidence/mortality/child-mortality/
(2) ALSG: Advanced Paediatric Life Support






