
Introduction
There are multiple differences between the circulatory system in the adult and the foetus.
As a brief overview of the adult system, on average there is around 5 litres of blood within the circulation, equating to around 8% of body weight. The cardiac output is approximately 5 litres/min, with 80% of circulating volume in the systemic veins, right side of the heart, and pulmonary circulation.
In the adult, deoxygenated blood returns to the right atrium via the vena cavae, and after passing through the right ventricle, the entire cardiac output passes via the pulmonary arteries to the lungs to enable gas exchange. Oxygenated blood then returns via the pulmonary veins to the left ventricle, passing through the left ventricle and allowing the entire cardiac output to enter the systemic circulation via the aorta.
The rest of this article will discuss the foetal circulation, both before and after birth.
Foetal Circulation Before Birth
The foetal circulation is significantly different from the adult circulation, since the lungs are not mature enough to enable gas exchange, so gas exchange instead occurs in the placenta. Moreover, the foetal cardiovascular system is adapted to ensure the most highly oxygenated blood is delivered to the myocardium and brain; this is achieved by preferential streaming of oxygenated blood and presence of intracardiac and extracardiac shunts.
Therefore, foetal circulation is usually defined as “duct dependent”. There are four key adaptations present in the foetal circulation: (1) umbilical arteries and vein, (2) ductus venosus, (3) foramen ovale, and (4) ductus arteriosus (Fig. 1)
At the Liver
Oxygenated blood from the placenta travels via the umbilical vein, which branches into the left and right umbilical veins at the liver.
The right umbilical vein provides oxygenated blood to the liver via the portal vein, whilst the left umbilical vein branches into the ductus venosus, which bypasses the liver to carry oxygenated blood directly into the inferior vena cava (IVC).
A mix of oxygenated (from ductus venosus) and deoxygenated (from liver and the rest of the body) blood then enters the right atrium via the IVC, also mixing with the SVC (50:50 split of blood entering the heart from SVC and IVC).
At the Heart and Lungs
As the lungs have no role in gas exchange, the pulmonary arterioles are in a hypoxic state. Hypoxia causes a pulmonary vasoconstriction, which in turn increases pulmonary vascular resistance and pressure within the pulmonary circulation. This means that in foetal circulation, unlike in the adult, the pressure is higher in the right side of the heart.
As a result, the right ventricular afterload increases, causing blood to preferentially shunt away from the right ventricular outflow tract, via the ductus arteriosus (between pulmonary artery and aorta) and foramen ovale (between right atrium and left atrium). Consequently, most of the blood bypasses the right ventricle and lungs altogether, entering the left atrium or directly into the aorta, to then be pumped around the systemic circulation. This allows relatively oxygen-rich blood to be pumped to the body.
The aorta bifurcates into the right and left common iliac arteries, which split further into the internal and external iliac arteries. Each of the internal iliac arteries give rise to an umbilical artery, which travel alongside the umbilical vein to bring deoxygenated blood back to the placenta. This cycle continues until birth.
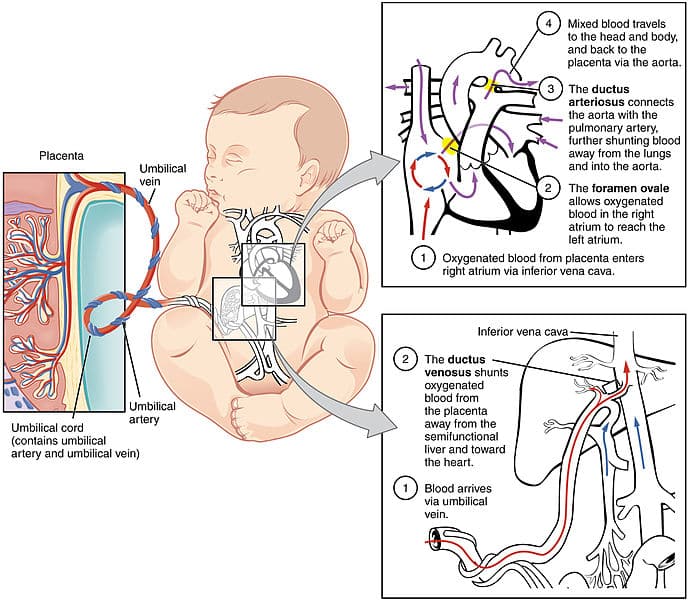
Figure 1 – Summary of the Foetal Circulation Prior to Birth
Foetal Circulation After Birth
After birth, air flows into the lungs to replace the water in the alveoli, resulting in a significant rise in oxygen levels in the lungs. Pulmonary vascular resistance falls due to reductions in hypoxic pulmonary vasoconstriction, meaning a lower pulmonary resistance and decreased afterload in the right side of the heart.
A change in pressure gradients between the left and right side of the heart results in closure of the foramen ovale (Fig. 2). Decrease in pulmonary pressure means that blood flow across the ductus arteriosus is also reversed, with blood initially shunted from the aorta to pulmonary artery. As oxygen levels rise, the smooth muscles in the walls of ductus arteriosus constrict, eventually closing completely* (forming the ligamentum arteriosum in adults).
After birth, the umbilical vessels constrict, forming the round ligament of the liver (umbilical vein), ligamentum venosum of the liver (ductus venosus), and superior vesical arteries (umbilical arteries).
*High levels of prostaglandin produced by the placenta also contribute to keeping the ductus arteriosus open in utero; after birth, as a result of separation of the placenta, prostaglandin levels also fall, further contributing to its closure
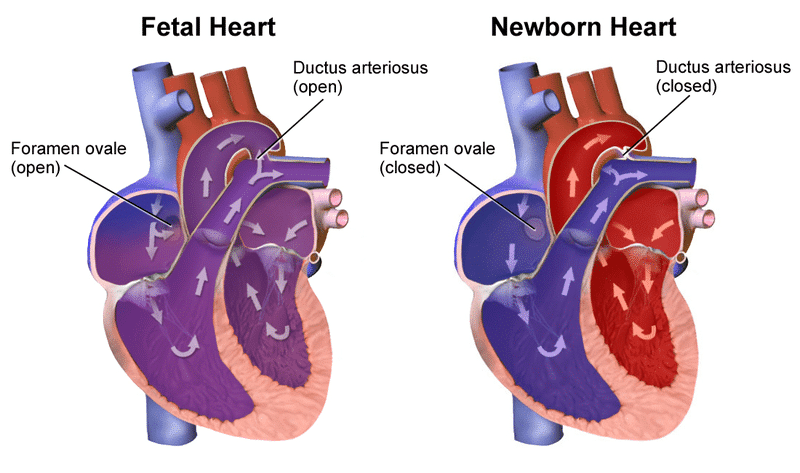
Figure 2 – Changes that occur to the Heart Following Birth
Foetal Haemoglobin
Foetal haemoglobin has a higher affinity for oxygen compared to maternal haemoglobin. This means foetal haemoglobin binds to oxygen more strongly and enables the transfer of oxygen from mother to foetus prenatally.
Foetal haemoglobin has an oxygen dissociation curve that is displaced to the left compared to adult haemoglobin (Fig. 3). As a result, for a given partial pressure of oxygen (pO2), the haemoglobin is more saturated than adult haemoglobin.
At birth, 80% haemoglobin remains in the foetal form, however this falls to 10% by four months of age. Infants continue to generate foetal haemoglobin for up to 6 months of age, which will diminish oxygen exchange between the vasculature and tissue throughout the body.
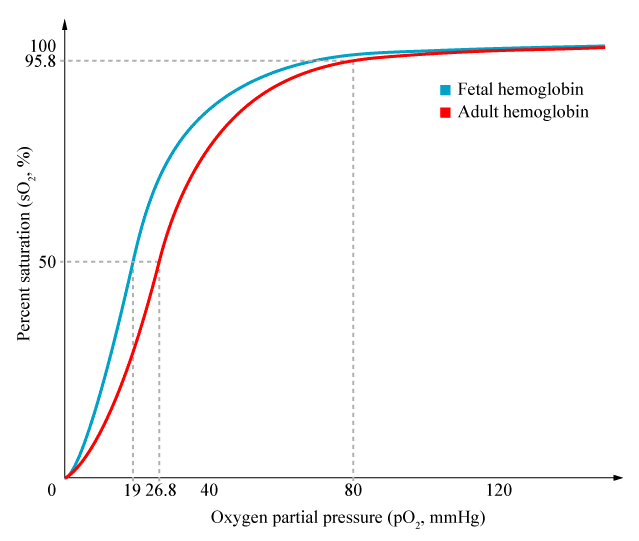
Figure 3 – Oxygen Dissociation Curve for Foetal and Adult Haemoglobin
Key Points
- The foetal circulation is significantly different from the adult circulation, since the lungs are not mature enough to enable gas exchange
- Foetal haemoglobin has a higher affinity for oxygen compared to maternal haemoglobin; this means foetal haemoglobin binds to oxygen more strongly and enables the transfer of oxygen from mother to foetus prenatally